
If you’ve ever Googled “tennis elbow treatment,” you’ve probably landed on a list that includes rest, anti-inflammatories, a brace, maybe a cortisone injection, and the vague instruction to “avoid aggravating activities until it settles down.” For a lot of people, that advice leads to months (or years) of pain that comes and goes – quiet while they’re resting, then back the moment they pick up a racquet or a heavy bag.
As an Exercise Physiologist, I see tennis elbow – more accurately called lateral epicondylalgia – constantly, and the pattern is almost always the same: people are told to rest and wait, the pain settles while they’re resting, and then it comes roaring back the moment they return to the activities that matter to them. That’s because rest doesn’t build tendon capacity. It just buys you time.
In this post, I want to walk you through exactly how I approach tennis elbow rehab: what the research actually says about injections and other passive treatments (spoiler: less than you’d think), how to use a simple pain scale to guide how hard you push, and the full 3-stage loading protocol I use to rebuild tendon capacity from the ground up.
| Hand + Wrist Foundations is launching soon – a 12-week, 3-phase program built specifically for tendon issues like tennis elbow, golfer’s elbow, and wrist pain. Join the waitlist here to be the first to know when it opens. |
What Is Tennis Elbow (Lateral Epicondylalgia)?
Tennis elbow refers to pain on the outside (lateral side) of the elbow, where the tendons of your forearm extensor muscles attach to a bony bump called the lateral epicondyle. These are the muscles that lift your wrist and fingers up – the ones you use every time you type, grip a steering wheel, lift a kettle, shake a hand, or hit a backhand.
Despite the ‘-itis’ in lateral epicondylitis (which technically means inflammation), most chronic cases aren’t primarily an inflammatory problem. They’re a tendinopathy – a breakdown in the structure of the tendon caused by load that has outpaced the tendon’s capacity to handle it, whether that’s from a sudden increase in racquet sport volume, a new job involving repetitive gripping or typing, or simply normal tendon aging combined with everyday use. Despite the name, plenty of people who’ve never picked up a racquet develop it from manual work, gardening, gaming, or computer use.
What Does the Evidence Say About Injections and Passive Treatments?
This is the section a lot of people skip, but it’s the one I think matters most – because it explains why an active, loading-based approach is where I focus my time, rather than chasing injections or passive modalities

According to PubMed, a 2010 systematic review and meta-analysis published in The Lancet pooled data from 41 randomised controlled trials and found that corticosteroid injections for lateral epicondylalgia produced a large reduction in pain in the short term compared with no treatment – but this effect reversed at the intermediate term (26 weeks) and long term (52 weeks), where patients who received no injection actually did better. In other words: a cortisone shot can make you feel better quickly, but it may leave you worse off a year down the track.
A 2014 systematic review of randomised controlled trials published in the journal Hand reached a similar conclusion – corticosteroid injections offered short-term pain relief but no demonstrable long-term benefit, while non-invasive passive treatments such as bracing, standard physical therapy, and shockwave therapy did not show a clear, definitive benefit for pain relief either. The same review noted that lateral epicondylitis is often a self-limiting condition, tending to resolve over 12 to 18 months even without treatment.
A 2015 Bayesian network meta-analysis published in the British Journal of Sports Medicine compared a range of injection therapies for lateral epicondylalgia – including corticosteroid, platelet-rich plasma (PRP), autologous blood, botulinum toxin, and prolotherapy – and concluded that while several showed a trend toward better effects than placebo, corticosteroid injection specifically was not recommended, and the evidence for the others was not yet strong enough to confidently recommend one over another.
A 2022 randomized double-blinded placebo-controlled study by Couppé et al (2022) published in The American Journal of Sports Medicine compared heavy slow resistance (HSR) training combined with either a corticosteroid injection, tendon needling, or placebo needling in patients with chronic lateral elbow tendinopathy. All three groups improved equally on pain and function scores after 12 weeks, but by 52 weeks, the corticosteroid group showed a tendency toward worse outcomes than the placebo group, including a significantly higher QuickDASH score (measuring how much difficulty the participants had had with arm/hand/shoulder function). The corticosteroid injection also produced a notable short-term reduction in tendon hypervascularization, but this didn’t translate into better grip strength or symptom relief. The takeaway: a properly dosed HSR program appears to drive the real improvement in tennis elbow, and adding a corticosteroid injection may actually undercut long-term results rather than enhance them.
And a 2022 overview of systematic reviews published in Healthcare looked at 25 systematic reviews covering 227 randomised controlled trials on lateral elbow pain. It found that conservative, multimodal approaches – things like exercise, manual therapy, and ultrasound – were the most commonly studied first-line treatments, with injections and surgery generally positioned as later options once conservative care had been tried.
Taken together, this is exactly why I think the evidence for injections and many passive treatments is, frankly, limited – particularly when it comes to long-term outcomes. They’re not necessarily ‘bad’ or never appropriate, but they don’t address the underlying issue: a tendon that needs progressive load to rebuild its capacity. That’s where the rest of this rehab plan comes in.
Using the Pain Scale to Guide Your Rehab
One of the biggest mistakes I see people make with tendon rehab is treating ‘no pain’ as the goal from day one. Some discomfort during loading exercises isn’t just okay – it’s often necessary for the tendon to adapt. The key is knowing how much is an acceptable amount, and that depends on where you’re starting from.
Here is the general rule I use:
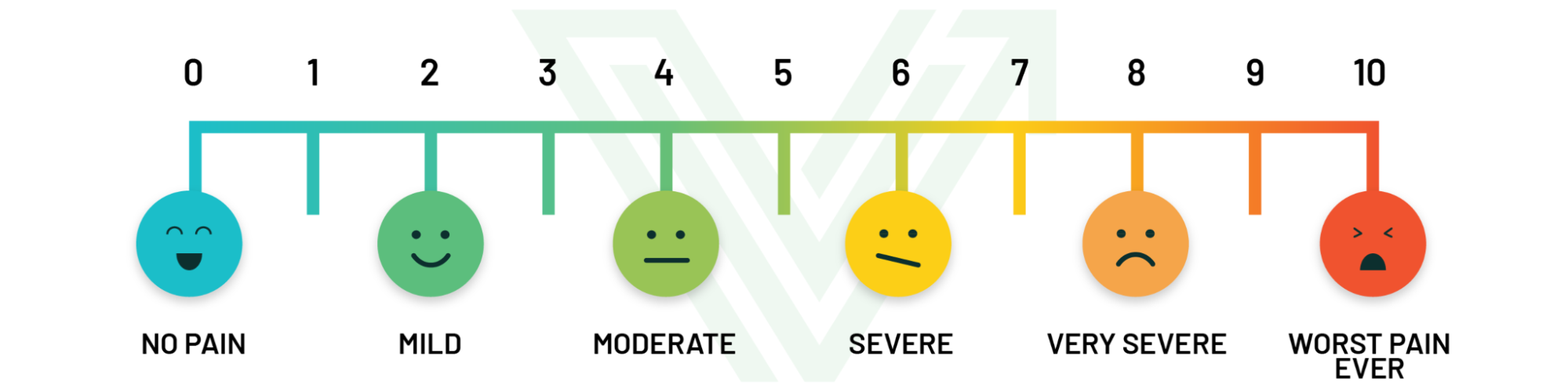
- If your pain at rest, or during normal daily activities, is relatively low (around 0-4 out of 10), then 3-5/10 pain during your rehab exercises is an acceptable starting point. This level of discomfort should settle back down within a few hours, and certainly by the next morning. If it doesn’t, that’s a sign the load was too much for where your tendon is at right now.
- If your pain at rest or during daily activities is already high (5-10/10), that’s a sign your tendon is more irritable, and pushing into 3-5/10 during exercise is likely to flare things up. In this case, drop the tolerable pain during rehab exercises right down to around 1/10, and build up gradually from there as your baseline pain settles.
The point of the pain scale isn’t to avoid discomfort altogether – it’s to make sure you’re loading the tendon enough to drive adaptation, without tipping it into a flare-up that sets you back. Checking in with this scale before, during, and the morning after each session is one of the simplest ways to self-regulate your rehab.
The 3-Stage Tendon Rehab Protocol
This is the framework I use for tendon rehab across the body, adapted here specifically for the wrist and elbow extensor tendons involved in tennis elbow. It’s broken into three stages, and the general idea is simple: calm things down without losing capacity, then rebuild strength, then prepare the tendon for the fast, reactive demands of sport and daily life.
You don’t necessarily move through these stages on a fixed timeline – you progress based on your symptoms, using the pain scale above as your guide.

Stage 1: Isometrics & Calming Things Down (Acute Phase)
General guidelines:
- Don’t “poke the bear”: modify painful movements rather than testing or pushing through pain to ‘see how it feels.’
- Consider anti-inflammatories for 1-2 weeks (used daily, under guidance from your doctor or pharmacist) if appropriate for you, especially if the condition involves enthesitis (inflammation of the tendon in the tubules in which it attaches to the bone) or if the pain is really limiting simple activities of daily living (dressing, making food, working, etc).
- Pain should not exceed 3/10 during or after activity.
- Daily isometrics for pain relief: 10-30 second holds, 2 minutes rest, 5 sets. Ideally, in the morning because tendinopathies typically feel worse in the morning and isometrics can offer an analgesic effect (naturally decreasing the pain immediately)
- Keep up pain-free strength training elsewhere – just avoid deep wrist flexion/extension, excessive gripping/compression, or heavy loads through the affected tendon.
- No stretching at this stage – tendons are sensitive to compression, and stretching the wrist extensors compresses the tendon against the bone.
- Monitor your pain the next day – if it’s increased, that’s a sign you’ve loaded too much.
Activity Modification:
- Avoid high-load gripping activities, racquet sports, and repetitive wrist extension tasks (e.g., screwdriving, hammering, heavy single-hand carrying) until your pain settles.
- In the gym, consider using straps to offload your grip a little. We use THESE ones and love them.
- Light use of the hand for daily tasks – typing, light grip, eating – is generally fine if it doesn’t aggravate symptoms.
- Modify gripping tasks where you can: use two hands instead of one, choose larger-diameter handles, switch hands for repetitive tasks, and avoid carrying heavy bags or shopping in the affected hand.
- Avoid provocative positions and movements – forceful gripping, wrist extension against resistance, and excessive stretching into wrist flexion.
- Avoid ‘testing’ the elbow by repeatedly checking if it still hurts – this is one of the most common ways people unintentionally keep a tendon irritated.
- Use a neutral wrist position (wrist straight, not flexed or extended) to start – for example, pressing the back of your hand into a table edge or against your other hand without moving the wrist.
- Keep training the rest of your body – pain-free movement is the priority.
- Modify any exercises that load the wrist extensors heavily (e.g., heavy rows, deadlifts with a hook or thick grip, pull-ups) to reduce grip demand or load.
- Avoid explosive or ballistic movements through the wrist and forearm for now.
Load Management & Recovery:
- Keep exercise-related pain at 3/10 or below.
- If symptoms persist despite the above, consider a short, temporary deload from the aggravating activity (this doesn’t mean stopping all activity – just reducing the specific load that’s driving symptoms).
- Downregulate your nervous system where you can – sleep, stress management, breathing exercises, and general relaxation all play a role in how irritable a tendon feels. This is where massage, acupuncture and manual therapy services can also help. You can find ours HERE.
Monitoring & Progression:
- The goal of Stage 1 is to get your pain settled to a manageable, predictable baseline while maintaining daily isometric loading.
- You’re ready for Stage 2 once your symptoms have settled and you can tolerate your isometrics and daily activities without a significant next-day flare.
Stage 2: Slow & Heavy Strength (with Continued Isometrics)
General guidelines:
- Progress load, not stretch – the focus here is building tendon and muscle capacity through controlled strength work, not flexibility.
- Avoid explosive or fast movements for now – keep loading slow and controlled.
- Monitor your morning pain levels – an increase is a sign you’ve progressed load too quickly.
- Be patient with your return to racquet sports or other high-demand activities – this stage is about building a foundation, not rushing back.
1. Activity Progression
- Gradually reintroduce gripping, lifting, and racquet-based activities – avoid sudden jumps in load or volume.
- If returning to racquet sports, start with shorter sessions and avoid playing on consecutive days initially.
- Continue avoiding excessive compression and stretching of the wrist extensors – progress through loading instead.
- Monitor next-day pain after any new activity or increase in volume.
2. Continued Isometric Loading
- Morning isometrics continue daily: 30 second holds, 2 minutes rest, 3-5 sets.
- Add a wrist extension isometric against light resistance (e.g., pressing the back of your hand against a table or resistance band) in addition to the neutral-position hold.
- Before racquet sports or heavy gripping tasks, use a short isometric “activation” hold for the wrist extensors as part of your warm-up.
- Evening isometrics can build up to 3-minute holds for muscular endurance.
- Optional: a light isometric grip hold before bed (squeezing a soft ball at low-to-moderate effort), keeping pain at or below 3/10.
3. Slow & Heavy Strength Progression
- Prioritise slow, controlled movements – nothing explosive yet.
- Load should be challenging but pain-free (or no more than 3/10): aim for 8 reps x 4 sets, 2-3 times per week.
- Use a controlled tempo – 3 seconds up 3 seconds down – with a 3 second hold in the middle if things are particularly flared up
- Exercise selection should cover the full range of motion and the muscles surrounding the elbow and wrist – for example, wrist extension and flexion curls, eccentric wrist extension, forearm pronation/supination, and grip strengthening.
4. Dynamic Stretching (Optional, If Tolerated)
- Only introduce dynamic wrist stretches if they don’t increase your pain afterward.
- Hold each stretch for 6-10 seconds.
- Stop immediately if you notice any increase in discomfort or symptoms.
Stage 3: Store & Release / Plyometric Phase
General guidelines:
- Gradually reintroduce higher-demand activities – controlled strength progressions and a return to full racquet sport volume.
- Begin introducing plyometric (fast, reactive) loading for the wrist and forearm.
- Pain should not exceed 3/10 during or after activity.
- Continue daily isometrics for pain control and tendon capacity – now at 15-45 second holds, 5 sets.
- Strength training remains slow and heavy, but you can begin introducing some fast, explosive strength work too.
Isometric Loading for Tendon Capacity (Daily):
- Morning isometrics: choose 1-2 wrist extensor isometric holds, 3-5 sets of 30+ seconds, 60 seconds rest.
- Evening isometrics: continue building toward 3-minute holds for muscular endurance.
- Incorporate two-handed and single-hand loaded holds (e.g., a farmer’s carry hold) for additional grip and forearm capacity.
Activity Progression & Sport Tolerance:
- Increase the frequency and duration of racquet sports or gripping-heavy activities gradually.
- Monitor for delayed pain – next-morning soreness is a sign the load was too high and needs to come back slightly.
- General conditioning (running, cycling, or other lower-body cardio) can continue throughout this process to maintain overall fitness while your forearm tendon progresses at its own pace.
Plyometrics:
- Begin introducing fast, stretch-shortening loading for the wrist extensors while monitoring next-day pain – for example, catching and releasing a lightly weighted ball with the wrist extending and absorbing the catch.
- Progress from slower, lighter catches to faster, higher-load catches, throws, or racquet drills that involve quick deceleration and direction change.
General Conditioning Progression:
- Gradually increase the volume and intensity of racquet sport sessions or other gripping-heavy activities, avoiding back-to-back high-load days early on.
- Progress overall training volume over roughly two weeks at a time, monitoring pain and next-day response as your guide.
Related Reading: 16 Key Things About Injured Tendons
If you want to go deeper on how tendons heal, why they behave the way they do under load, and what actually helps them get stronger, I’d really recommend reading 16 Key Things About Injured Tendons. It covers a lot of the ‘why’ behind the approach in this post, and it applies to tendon injuries well beyond just tennis elbow.

Ready to Build a Plan With Us?
Tennis elbow can feel like it drags on forever when the only tools being used are rest, bracing, and the occasional injection. But tendons respond to load – and with the right progression, most people can get back to the racquet sports, lifting, and everyday activities they’ve been avoiding.
If you’re dealing with tennis elbow, golfer’s elbow, wrist pain, or any other hand and wrist tendon issue, our Hand + Wrist Foundations program is a 12-week, 3-phase programming series built around exactly this kind of progressive loading approach. Join the waitlist here to be the first to know when it opens.
References
Cardoso, T. B., Pizzari, T., Kinsella, R., Hope, D., & Cook, J. L. (2019). Current trends in tendinopathy management. Best Practice & Research Clinical Rheumatology, 33(1), 122–140. https://doi.org/10.1016/j.berh.2019.02.001
Cook, J. L., & Purdam, C. R. (2009). Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine, 43(6), 409–416. https://doi.org/10.1136/bjsm.2008.051193
Cook, J. L., & Purdam, C. R. (2013). The challenge of managing tendinopathy in competing athletes. British Journal of Sports Medicine, 48(7), 506–509. https://doi.org/10.1136/bjsports-2012-092078
Coombes, B. K., Bisset, L., & Vicenzino, B. (2010). Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: A systematic review of randomised controlled trials. The Lancet, 376(9754), 1751–1767. https://doi.org/10.1016/S0140-6736(10)61160-9
Couppé, C., Døssing, S., Bülow, P. M., Siersma, V. D., Zilmer, C. K., Bang, C. W., Høffner, R., Kracht, M., Hogg, P., Edström, G., Kjaer, M., & Magnusson, S. P. (2022). Effects of heavy slow resistance training combined with corticosteroid injections or tendon needling in patients with lateral elbow tendinopathy: A 3-arm randomized double-blinded placebo-controlled study. The American Journal of Sports Medicine. Advance online publication. https://doi.org/10.1177/03635465221110214
Di Filippo, L., Vincenzi, S., Pennella, D., & Maselli, F. (2022). Treatment, diagnostic criteria and variability of terminology for lateral elbow pain: Findings from an overview of systematic reviews. Healthcare, 10(6), Article 1095. https://doi.org/10.3390/healthcare10061095
Dong, W., Goost, H., Lin, X.-B., Burger, C., Paul, C., Wang, Z.-L., Kong, F.-L., Welle, K., Jiang, Z.-C., & Kabir, K. (2015). Injection therapies for lateral epicondylalgia: A systematic review and Bayesian network meta-analysis. British Journal of Sports Medicine, 50(15), 900–908. https://doi.org/10.1136/bjsports-2014-094387
Escriche-Escuder, A., Casaña, J., & Cuesta-Vargas, A. I. (2020). Load progression criteria in exercise programmes in lower limb tendinopathy: A systematic review. BMJ Open, 10(11), e041433. https://doi.org/10.1136/bmjopen-2020-041433
Paxton, J. Z., Hagerty, P., Andrick, J. J., & Baar, K. (2012). Optimizing an intermittent stretch paradigm using ERK1/2 phosphorylation results in increased collagen synthesis in engineered ligaments. Tissue Engineering Part A, 18(3–4), 277–284. https://doi.org/10.1089/ten.tea.2011.0336
Sims, S. E. G., Miller, K., Elfar, J. C., & Hammert, W. C. (2014). Non-surgical treatment of lateral epicondylitis: A systematic review of randomized controlled trials. Hand, 9(4), 419–446. https://doi.org/10.1007/s11552-014-9642-x
Steffen, D., Mienaltowski, M. J., & Baar, K. (2022). Scleraxis and collagen I expression increase following pilot isometric loading experiments in a rodent model of patellar tendinopathy. Matrix Biology, 109, 34–48. https://doi.org/10.1016/j.matbio.2022.03.006

More About The Author
Carla Robbins, MSc Exercise Physiology — Co-Founder, Vital Performance Care
Carla holds an Undergraduate Degree in Exercise Physiology from the University of Calgary and a Master’s in Exercise Physiology (2016). She has worked with the Canadian Sport Institute and co-founded Vital Performance Care with Dr. Amy MacKinnon inside Eau Claire Athletic Club in Calgary. Carla specializes in fitness testing, endurance training, and strength and conditioning for everyday and high-performance athletes.


