
We see it all the time: someone comes in with pain on the inside of their elbow, and the first thing they say is, “I don’t even play golf.”
Good. Because golfer’s elbow — medial epicondylitis, or more accurately, medial epicondylitis — has almost nothing to do with golf.
It’s a load tolerance problem. And understanding that distinction is what changes everything about how you manage it.
What Is Golfer’s Elbow, Really?
Golfer’s elbow refers to pain and tenderness on the medial epicondyle — the bony bump on the inside of your elbow — where the wrist flexors and forearm pronators attach. Technically it’s a tendinopathy: a breakdown in the structural integrity of the tendon at that attachment site caused by accumulated stress that outpaces the tissue’s ability to adapt.
The classic story is repetitive gripping, wrist flexion, and forearm pronation without enough recovery or progressive adaptation. The tendon gets overloaded. It starts to degrade. Pain follows.
(For an article I wrote specifically on the 16 things you need to know about tendons – read more HERE). Got Tennis Elbow instead of Golfer’s Elbow – read our siamese twin article HERE!
“Golfer’s elbow” is just the sport that happened to make it famous. In my practice, I see it far more often in:
- Mountain bikers and dirt bikers
- Rock climbers and obstacle course athletes
- CrossFitters and weightlifters (especially during high-volume deadlift or pull-up phases)
- Office workers who type and mouse for 8+ hours a day
- Tradespeople — plumbers, electricians, carpenters
- Hockey players (from stick handling) and racket sport athletes
- New gym-goers who jumped into grip-heavy training before their tendons were ready
If you grip things for a living or a sport, you are a candidate. Golf is just one of many entry points.
What Does Golfer’s Elbow Feel Like?
The pain from golfer’s elbow sits on the inside of your elbow — specifically at the medial epicondyle, the bony bump you can feel on the inner side of your elbow joint. That’s where the tendons that control wrist flexion and forearm rotation attach, and when those tendons are overloaded, that spot becomes the epicentre of the problem.
Common things people notice:
- Aching or tenderness on the bony bump on the inside of your elbow
- Pain when gripping, squeezing, or lifting — even light objects like a coffee cup
- Weakness in your grip or forearm, especially when trying to hold something with your arm extended
- Discomfort during wrist curls, forearm exercises, or pulling movements like rows or pull-ups
- A dull ache that lingers at rest in more irritated cases
- Occasional referred discomfort that travels down into the forearm
If this sounds familiar, it’s worth getting some guidance. As exercise physiologists, we can’t diagnose your pain or clear you for red flags like neuropathic symptoms – that’s outside our scope. But we can use exercise to help you safely reduce load, rebuild tolerance, and progressively work back toward the things you love – whether that’s golf, the gym, or just getting through your workday without that ache flaring up. If you’d like to work with one of our CEPs, you can book a session HERE in Calgary.
Why Rest Alone Doesn’t Fix It
When most people feel that ache on the inside of their elbow flare up, the instinct is predictable: rest it, ice it, pop some NSAIDs, maybe book a massage. And those things can help you feel better in the short term. But they don’t fix the underlying problem – because they’re not speaking the tendon’s language.
Tendons communicate through load. That’s how they receive the signal to remodel, adapt, and get stronger. Think of it this way: if you and I only speak English, and someone walks up and starts speaking French, nothing gets communicated – no matter how good their intentions are. Rest, ice, and NSAIDs are speaking French to a tissue that only understands English. Without the right mechanical input, the tendon simply can’t receive the message to heal.
Here’s the mistake most people make: they rest, the pain goes away, they go back to doing exactly what they were doing, and within weeks the pain is back.
That cycle happens because rest removes load – but it doesn’t build load tolerance. The tendon never got stronger. It just got a break.
Tendons respond to progressive mechanical stress. They remodel when you load them appropriately, repeatedly, over time. Rest alone doesn’t create that signal. In fact, prolonged rest can reduce tendon stiffness and slow recovery.
The modern approach – and the one we use at Vital – is to find the level of load the tendon can currently tolerate, and then systematically increase it. Pain-free does not mean strong. Strong means strong.
How do you know if you’re strong? We have devices like the Force Frame and Dynamo Plus to test it. Here’s an example of some of the strength testing we recently did on the elbow/forearm muscles which helps us set a baseline, check for asymmetries, and see how strong you are compared to your age/gender (note: 83pct is the 83rd percentile – meaning this person was stronger than 83% of people his gender and age).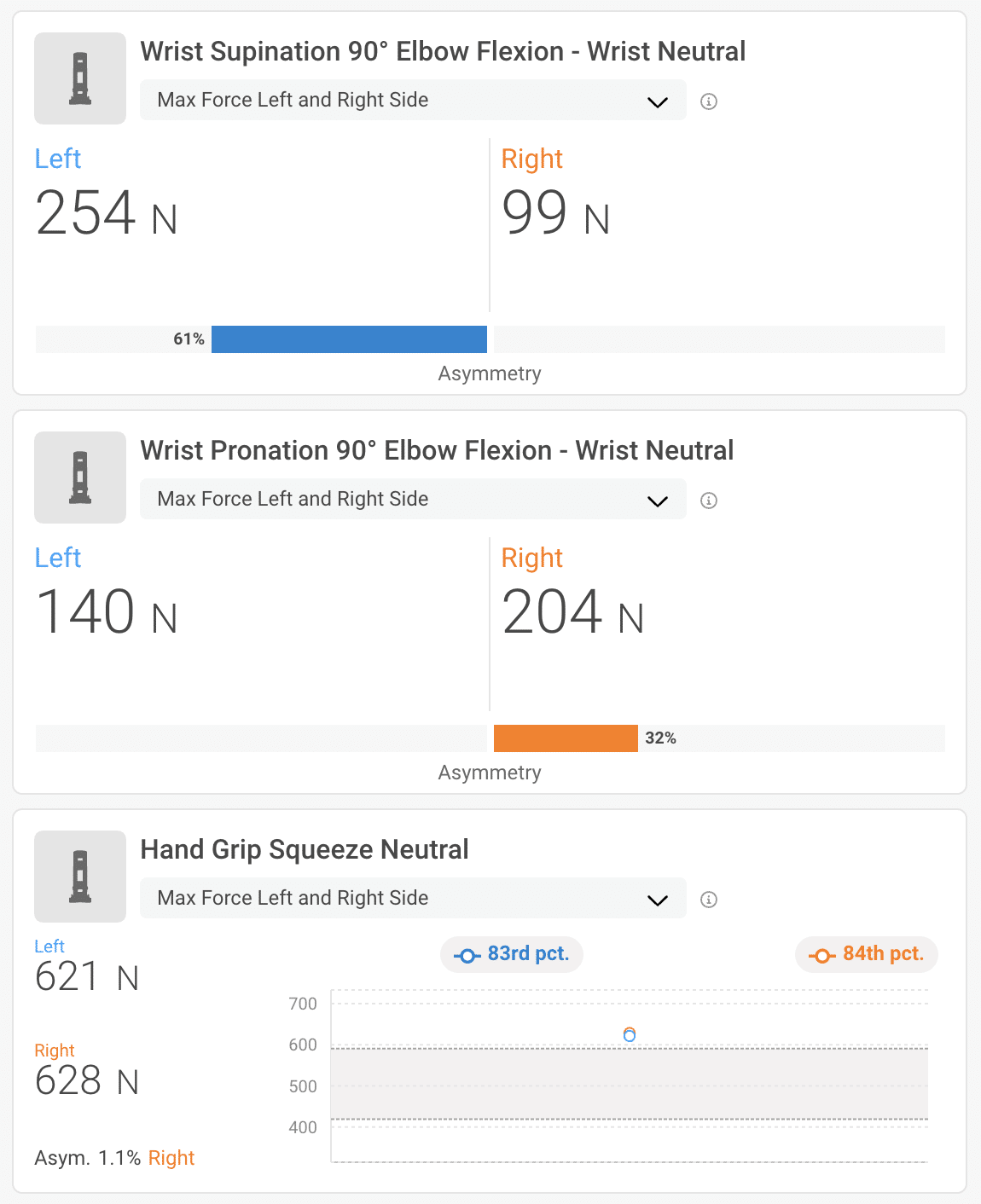
The Exercise Physiology Approach: Building Load Tolerance
As an exercise physiologist, my job isn’t to manually “treat” golfer’s elbow in a clinical sense – that’s what our physio and chiro team is for. My job is to figure out what your wrist flexors, forearm pronators, and grip can actually handle right now, and build a progressive program from there.
While most people just rest, ice, and wait when they have a flared up elbow, what we recommend is starting with isometrics and increasing the tolerance and capacity of the tissue.

That program typically moves through three stages:
Stage 1: Isometric Loading (Pain Education + Tendon Activation)
We start with isometric holds because they produce strong analgesic effects – isometrics can directly reduce tendon pain – and they let us load the tissue without movement. This is especially useful when even basic wrist flexion is irritable.
A great starting point is the ISO supinated hold with wrist flex: seated, forearm supported on the knee, holding a dumbbell or thick implement (PVC pipe, phat grip, or a protein container used as a hub grip) with the elbow at 90 degrees in supination, and adding a gentle wrist flexion bias. Hold 30-45 seconds, 3–4 sets. The load should produce mild discomfort (3–4/10) but not spike or linger afterward.
We’ll also vary wrist position – neutral, ulnar deviation, extended – to identify which angles tolerate load best and build from there. The goal isn’t to avoid all discomfort. It’s to find the right amount of it. This is exactly the kind of systematic entry-point mapping that Grant and I have been working through as we develop Hand+Wrist Foundations – figuring out which exercises suit which presentations so we can build clear progressions for people to follow.
Stage 2: Isotonic Wrist Flexor Curls Through Full Range
Once isometrics are well-tolerated, we move into slow, controlled wrist flexor curls through full range with an emphasis on the eccentric (lowering) phase – where the most tendon remodelling signal is generated.
Single-arm DB wrist flexor curl – forearm anchored on the knee, palm up, slow tempo. We vary grip type progressively: standard grip first, then phat grip (thicker implement), then pinch grip, then hub grip (holding a protein container by the lid). Each variation shifts the demand slightly and keeps adaptation happening. These progressions seem deceptively simple. The results aren’t.
Wrist roller – loaded progressively with increasing weight. This is an underrated tool for medial elbow issues because it loads both the wrist flexors and extensors through a full pronation-supination arc simultaneously. You can build one easily with PVC pipe, rope, and a weighted bag. Start very light.
90-degree elbow supinated curl – arm held at 90 degrees, palm up, slow eccentric, with an optional finger roll at the bottom to engage the distal tendon attachment more specifically. DB or barbell, seated.
Stage 3: Pronation Loading and Grip Strength
Here’s what often gets missed in medial elbow rehab: the pronator teres shares that medial epicondyle attachment. If you’re only loading wrist flexion and ignoring pronation strength, you’re leaving a significant piece of the recovery on the table.
SA pronation curl – forearm supported on the knee, rotating from supination into pronation through the movement. Using a longer implement – a hockey stick, a club, a longer dumbbell – creates a longer lever arm and more rotational demand with the same absolute load. This is exactly the sport-specific progression that matters for hockey players, golfers, and racket sport athletes.
Reverse curl – forearm pronated, wrist in a neutral or slightly extended position through the curl. This targets the wrist extensors – the antagonists to the structures typically involved in golfer’s elbow – and builds the co-contraction balance that protects the medial elbow under dynamic load.
Grip work – both crush grip (lax ball, Captains of Crush, thick barbell hangs) and sustained isometric holds. Grip strength is one of the most trainable and most neglected variables in elbow tendinopathy recovery. Stronger grip means better force distribution across the forearm, which means less concentrated load sitting right at the epicondyle.
Hand/Wrist Foundations Is Coming
I want to be honest about something: most people’s wrist and hand training is an afterthought. We focus on the big movements, the compound lifts, the sport-specific drills. The hand is just the thing holding the bar.
But grip is the first link in every kinetic chain that involves an implement – hockey stick, golf club, barbell, keyboard, climbing hold. When that link is weak or undertrained, everything upstream compensates. Golfer’s elbow is often just the visible consequence of a chain that’s been asking the wrong link to carry too much for too long.
Grant and I have been developing a structured Hand/Wrist Foundations program here at Vital — built on the same framework as Shoulder Foundations: progressive loading phases, phase-gated testing benchmarks, and specific tracks for pain management, performance, and longevity. It’s designed for everyone from office workers with chronic wrist tension to climbers who want to train grip the right way to hockey players who want their stick-hand to be a genuine strength.
Hand/Wrist Foundations is planned for launch later this year. If you’ve been dealing with recurring hand, wrist, or elbow issues – or if you simply want to build real resilience in this area before a problem develops – reach out to our team and we’ll make sure you’re first to hear when it opens.
Ready to Stop Guessing?
If medial elbow pain keeps coming back, more rest is rarely the answer. Building the right load tolerance, in the right sequence, is.
Our exercise physiology team at Vital Performance Care can assess where your grip and wrist flexor capacity actually stands, design a program that builds from there, and coordinate with our clinical team when something structural needs to be addressed first.

More About The Author
Carla Robbins, Co-Founder of Vital Performance Care
Carla’s journey into the world of endurance training, strength and conditioning, and exercise physiology began with her Undergraduate Degree in Exercise Physiology at the University of Calgary and continued into her graduation with a Master’s in Exercise Physiology in 2016. Between working for the Canadian Sports Institute to the creation of her company Vital Strength and Physiology Inc (now Vital Performance Care), Carla is driven by a desire to find better ways to address complex cases in professional and everyday athletes and individuals.


